
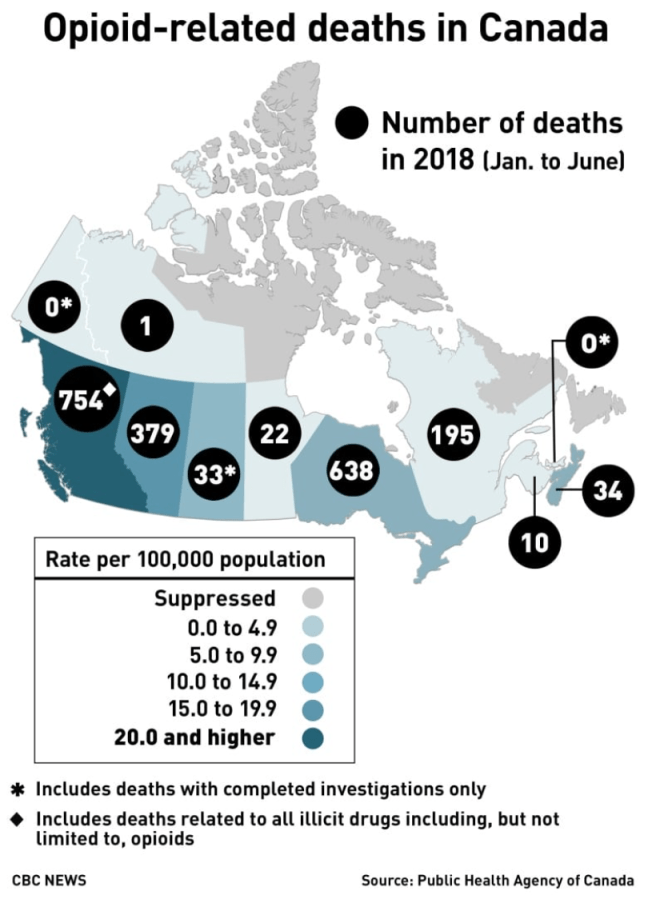
More North Americans die of opioid abuse than in traffic accidents. In 2017, 3,987 Canadians died from opioid overdoses. In the U.S., where widespread opiate and opioid abuse started earlier, the number of deaths topped 72,000. [Ed.: the terms opiate and opioid initially were used to differentiate between drugs derived from opium and synthesized variants. Opioid has become the umbrella term.]
Opioid abuse takes many forms, says a prominent Quebec pain control and addiction specialist. “Patients with prescriptions sell their meds or fail to store them safely.”
He sees adolescents, especially those who consume THC, buying opioids and becoming addicted. “THC consumed in adolescence alters brain structure and chemistry, leading to a decrease in verbal memory, especially if the person is also battle ADHD, anxiety or mood swings. Then they end up self-medicating with THC.”
How widespread is opioid abuse? He cites a study of 570,000 opioid-unaware patients receiving post-operative opioids who were followed for 2.7 years. “One per cent overused or abused, but with serious consequences […] The risk of abuse doubles with every prescription renewal, even one, regardless of dosage.” His conclusion: “Opioids should be prescribed in small doses over the short term, not repeatable.”
My source asked that I not identify him. His campaign to sensitize patients and healthcare bureaucrats to the risks of opioids has led to clashes with regulatory bodies responsible for ensuring the health and safety of patients. Instead, he says, these bodies act as if their sole intent is to ensure that alternatives such as cannabidiol (CBD) are hard to prescribe, obtain and assess for efficacy while giving the opioid industry free rein to do business as usual despite clear evidence of an epidemic of abuse.
I asked him whether opioids are effective, non-addictive painkillers when used as prescribed.
“I came to realize that my patients taking opioids for pain relief were fat, lazy, sweaty, non-functional — and still in pain,” he replied. The condition is called opioid-induced hyperalgesia, characterized by a paradoxical response whereby a patient receiving opioids for the treatment of pain could actually become more sensitive to certain painful stimuli.
Urinalysis and close questioning led him to conclude some of his patients were trading their prescribed drugs for more powerful alternatives on the black market. Others were selling all or part of their prescribed drugs for cash. His doctor-patient relationship prevented him from turning them over to the police. The response from the Collège des médecins du Québec (CMQ)? Stop prescribing.
Since his aha! moment, he has pioneered in the prescribing of cannabinoids in the treatment of chronic neuropathic pain. He also seeks to educate, offering two-hour seminars to healthcare professionals during which he dispels misconceptions about cannabinoids and explains the chemistry and psychology of neuropathic pain. (Indicative of an awakening taking place within the industry, his lectures are sponsored by opioid producers Purdue and Janssen.)
He scrupulously maintains an arm’s-length relationship with Canada’s get-rich-quick cannabis industry. “I didn’t invest because I want to remain credible,” he told me in November. “It’s a huge field and it’s just starting…I saw it coming because the current treatments for neuropathic pain are not working.” Big Pharma knows it, federal and provincial regulators know it, doctors and pharmacists know it, he adds, but that knowledge isn’t being shared with the patient.
It’s equally clear to him that unless the medical cannabis industry can demonstrate the science to support efficacy claims, the industry can’t advance. “There’s a real lack of understanding of [the body’s own endocannabinoids and how they act on our pain receptors]. Unless there’s a scientific basis, there’s no research money.” Without research on a proposed substance’s medical indications, attenuating effects, optimum dosage and clinical trials, Health Canada won’t issue a Drug Identification Number (DIN), the basis on which a drug can be prescribed for a specific use and covered by public or private drug insurance.
Theoretically, any licenced Canadian doctor has been able since 2013 to write a prescription for medical marijuana and its derivatives without the patient having to enrol in a clinical trial. Because of the determined efforts of the Collège des médecins du Québec, it’s easier to buy black-market or grey-market cannabis than it is to find a Quebec GP willing to write a prescription.
As of April 1, 2014, cannabis could only be prescribed in Quebec “within a research framework,” as it is not a medically recognized treatment. Quebec patients with the financial wherewithal had the option of consulting one of a growing number of private pain clinics. Those without the means were given the choice of buying products online (with no guarantee of purity or dosage consistency) or from First Nations distributors (the Tyendinaga Mohawk Nation south of Belleville has 57 outlets selling medical and recreational cannabis of varying potency and quality). Until Quebec’s pot police ordered them to stop, the province’s pet stores were selling out their supplies of veterinary-quality CBD to arthritic oldsters of another species.
However, Quebec’s insistence on patients having to enrol in clinical trials may have given cannabinoid researchers a leg up. In May 2015, the world’s first research database on the use of cannabis for medical purposes, the Quebec Cannabis Registry (www.registrecannabisquebec.com) was launched under the auspices of the Research Institute of the McGill University Health Centre (RI-MUHC) and the Canadian Consortium for the Investigation of Cannabinoids (CCIC).
The Registry’s creators set a goal of 3,000 participants over a 10-year period. (The Registry stopped taking registrants in the fall of 2018 after enrolling the 3,000.) It curates clinical data from patients, sites and clinics throughout Quebec; each participant must agree to provide data for four years after recruitment. Any licensed doctor practising in the province wishing to authorize cannabis for their adult patients could enrol participants in the registry.
The CMQ sought to denigrate the Registry, claiming it doesn’t satisfy the criteria of true scientific research and therefore can’t demonstrate that cannabinoids offer a solid alternative to opioids for chronic pain relief. However, most I spoke to believe that research eventually will demonstrate that provincial pharmeconomies can save millions by replacing ineffective, addicting opioids and other prescription drugs with cannabinoids. In the end, it’s a cost-benefit analysis. What’s an overdose death worth? What’s the price tag on addiction? I understand the need for skepticism and caution but I find it incredible that in Canada, medical cannabis isn’t further ahead.
During a trip to Italy last fall, I was blown away by the percentage of Italians who use cannabidiol for pain relief. CBD is widely available throughout Rome, Florence, Milan and most larger cities. Italians who would never dream of smoking to get buzzed use CBD to treat arthritis, chronic pain, anxiety, insomnia and a list of inflammatory and autoimmune disorders. Significantly, Italy does not appear to have an opioid addiction problem.
The CBD sold in Rome was manufactured in Holland and certified 99% pure, which to my experience covering this issue is questionable.
While unlicenced extraction appears to be a crime nationally, one Quebec cannabidiol extractor told me he’s sourcing his CBD from non-psychoactive indica (hemp) plants. The active ingredient can be extracted with various easily available solvents. Ottawa’s legalization legislation, Bills C-45 and C-46, didn’t deal with this other than to stipulate that there would be a year’s delay before consumeables and edibles are legalized. At an industry conference last spring, several major players told me tell me the non-THC demand will dwarf recreational and they’re happy to have the time to source CBD precursors and develop delivery systems.
