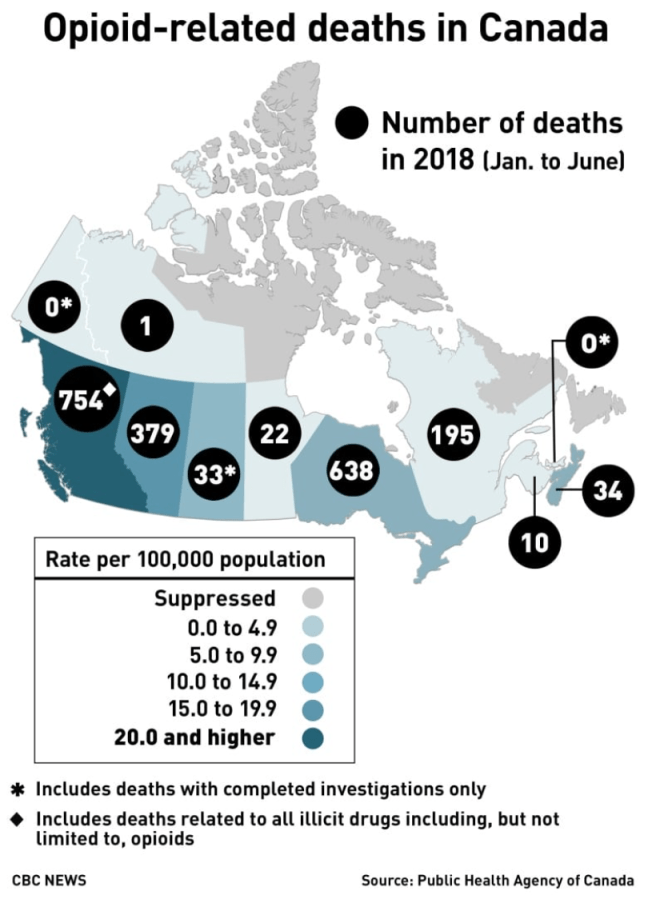
Canada’s chief public health officer Dr. Theresa Tam calls for safer opioids as she announces the death toll for the first half of 2018.
More North Americans die of opioid abuse than in traffic accidents. In 2017, 3,987 Canadians died from opioid overdoses. In the U.S., where widespread opiate and opioid abuse started earlier, the number of deaths topped 72,000. [Ed.: the terms opiate and opioid initially were used to differentiate between drugs derived from opium and synthesized variants. Opioid has become the umbrella term.]
Opioid abuse takes many forms, says a prominent Quebec pain control and addiction specialist. “Patients with prescriptions sell their meds or fail to store them safely.”
He sees adolescents, especially those who consume THC, buying opioids and becoming addicted. “THC consumed in adolescence alters brain structure and chemistry, leading to a decrease in verbal memory, especially if the person is also battle ADHD, anxiety or mood swings. Then they end up self-medicating with THC.”
How widespread is opioid abuse? He cites a study of 570,000 opioid-unaware patients receiving post-operative opioids who were followed for 2.7 years. “One per cent overused or abused, but with serious consequences […] The risk of abuse doubles with every prescription renewal, even one, regardless of dosage.” His conclusion: “Opioids should be prescribed in small doses over the short term, not repeatable.”
My source asked that I not identify him. His campaign to sensitize patients and healthcare bureaucrats to the risks of opioids has led to clashes with regulatory bodies responsible for ensuring the health and safety of patients. Instead, he says, these bodies act as if their sole intent is to ensure that alternatives such as cannabidiol (CBD) are hard to prescribe, obtain and assess for efficacy while giving the opioid industry free rein to do business as usual despite clear evidence of an epidemic of abuse.
I asked him whether opioids are effective, non-addictive painkillers when used as prescribed.
“I came to realize that my patients taking opioids for pain relief were fat, lazy, sweaty, non-functional — and still in pain,” he replied. The condition is called opioid-induced hyperalgesia, characterized by a paradoxical response whereby a patient receiving opioids for the treatment of pain could actually become more sensitive to certain painful stimuli.
Urinalysis and close questioning led him to conclude some of his patients were trading their prescribed drugs for more powerful alternatives on the black market. Others were selling all or part of their prescribed drugs for cash. His doctor-patient relationship prevented him from turning them over to the police. The response from the Collège des médecins du Québec (CMQ)? Stop prescribing.
Since his aha! moment, he has pioneered in the prescribing of cannabinoids in the treatment of chronic neuropathic pain. He also seeks to educate, offering two-hour seminars to healthcare professionals during which he dispels misconceptions about cannabinoids and explains the chemistry and psychology of neuropathic pain. (Indicative of an awakening taking place within the industry, his lectures are sponsored by opioid producers Purdue and Janssen.)
He scrupulously maintains an arm’s-length relationship with Canada’s get-rich-quick cannabis industry. “I didn’t invest because I want to remain credible,” he told me in November. “It’s a huge field and it’s just starting…I saw it coming because the current treatments for neuropathic pain are not working.” Big Pharma knows it, federal and provincial regulators know it, doctors and pharmacists know it, he adds, but that knowledge isn’t being shared with the patient.
It’s equally clear to him that unless the medical cannabis industry can demonstrate the science to support efficacy claims, the industry can’t advance. “There’s a real lack of understanding of [the body’s own endocannabinoids and how they act on our pain receptors]. Unless there’s a scientific basis, there’s no research money.” Without research on a proposed substance’s medical indications, attenuating effects, optimum dosage and clinical trials, Health Canada won’t issue a Drug Identification Number (DIN), the basis on which a drug can be prescribed for a specific use and covered by public or private drug insurance.
Theoretically, any licenced Canadian doctor has been able since 2013 to write a prescription for medical marijuana and its derivatives without the patient having to enrol in a clinical trial. Because of the determined efforts of the Collège des médecins du Québec, it’s easier to buy black-market or grey-market cannabis than it is to find a Quebec GP willing to write a prescription.
As of April 1, 2014, cannabis could only be prescribed in Quebec “within a research framework,” as it is not a medically recognized treatment. Quebec patients with the financial wherewithal had the option of consulting one of a growing number of private pain clinics. Those without the means were given the choice of buying products online (with no guarantee of purity or dosage consistency) or from First Nations distributors (the Tyendinaga Mohawk Nation south of Belleville has 57 outlets selling medical and recreational cannabis of varying potency and quality). Until Quebec’s pot police ordered them to stop, the province’s pet stores were selling out their supplies of veterinary-quality CBD to arthritic oldsters of another species.
However, Quebec’s insistence on patients having to enrol in clinical trials may have given cannabinoid researchers a leg up. In May 2015, the world’s first research database on the use of cannabis for medical purposes, the Quebec Cannabis Registry (www.registrecannabisquebec.com) was launched under the auspices of the Research Institute of the McGill University Health Centre (RI-MUHC) and the Canadian Consortium for the Investigation of Cannabinoids (CCIC).
The Registry’s creators set a goal of 3,000 participants over a 10-year period. (The Registry stopped taking registrants in the fall of 2018 after enrolling the 3,000.) It curates clinical data from patients, sites and clinics throughout Quebec; each participant must agree to provide data for four years after recruitment. Any licensed doctor practising in the province wishing to authorize cannabis for their adult patients could enrol participants in the registry.
The CMQ sought to denigrate the Registry, claiming it doesn’t satisfy the criteria of true scientific research and therefore can’t demonstrate that cannabinoids offer a solid alternative to opioids for chronic pain relief. However, most I spoke to believe that research eventually will demonstrate that provincial pharmeconomies can save millions by replacing ineffective, addicting opioids and other prescription drugs with cannabinoids. In the end, it’s a cost-benefit analysis. What’s an overdose death worth? What’s the price tag on addiction? I understand the need for skepticism and caution but I find it incredible that in Canada, medical cannabis isn’t further ahead.
During a trip to Italy last fall, I was blown away by the percentage of Italians who use cannabidiol for pain relief. CBD is widely available throughout Rome, Florence, Milan and most larger cities. Italians who would never dream of smoking to get buzzed use CBD to treat arthritis, chronic pain, anxiety, insomnia and a list of inflammatory and autoimmune disorders. Significantly, Italy does not appear to have an opioid addiction problem.
The CBD sold in Rome was manufactured in Holland and certified 99% pure, which to my experience covering this issue is questionable.
While unlicenced extraction appears to be a crime nationally, one Quebec cannabidiol extractor told me he’s sourcing his CBD from non-psychoactive indica (hemp) plants. The active ingredient can be extracted with various easily available solvents. Ottawa’s legalization legislation, Bills C-45 and C-46, didn’t deal with this other than to stipulate that there would be a year’s delay before consumeables and edibles are legalized. At an industry conference last spring, several major players told me tell me the non-THC demand will dwarf recreational and they’re happy to have the time to source CBD precursors and develop delivery systems.
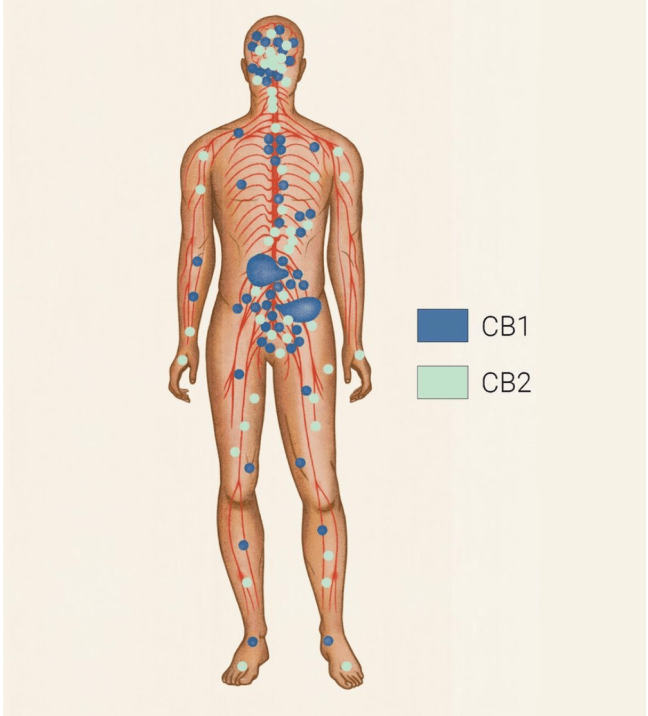
Human endocannabinoid receptors CB1 and CB2. Receptor sites are found in many organs and areas of the body, but CB1 receptors are primarily located in the central nervous system, which includes the brain. CB2 receptors are found primarily in the immune system. Cannabinoids THC and CBD interact with these receptor sites like our endocannabinoids do. (from the Ontario Cannabis Stores website (https://ocs.ca/blogs/how-cannabis-works/endocannabinoid-system).)
In November 2018 I was diagnosed with advanced osteoarthritis of the left hip. I’m scheduled to see a specialist in early February, with a surgical date dependent on the surgeon’s hospital OR schedule. According to the Canadian Institute for Health Information, I have an 83% chance of getting my hip replacement within 182 days of my referral.
In the meantime, I walk with a cane or ski pole. The only exercise left to me is swimming. My osteopath has succeeded in reducing associated sciatic pain but walking, standing, sitting and lying down are painful, often acutely. I can no longer control the pain with NSAIDs. I refuse to consider opioids because of their risks.
On the advice of my GP I enrolled in a clinical trial conducted by the Registre de cannabis du Quebec, the Quebec Cannabis Registry. I take 1.5 ml of prescribed cannabidiol oil under my tongue twice daily. CBD reduces the pain’s intensity, allowing me to get on with life. It takes approximately 90 minutes for the dosage to take effect.
Because everyone’s endo-cannabinoid receptors are unique, there is no such thing as a universal optimal dose or CBD/THC balance. Instead, one embarks on a trial-and-error process of finding one’s optimal dosage. Every refill arrives with a Health Canada fact sheet urging the beginner to start low and go slow in increasing one’s dosage.
My pain specialist prescribed Spectrum Yellow, 20% CBD and less than 1% THC. I’ve been keeping a daily journal on my results and observed side effects. On the plus side: my pain is reduced to a manageable dull ache, I enjoy deeper, more restful sleep, a reduced appetite (a positive because my GP says I have to lose 10 pounds or I’ll be using a walker), regularity, and heightened senses of smell and taste. Less welcome are the dry mouth and eyes and a loss of enjoyment for alcohol. I’ve also noticed interactions with coffee (too much or too little triggers fleeting headaches) and a tendency to slight depression if I don’t drink a lot more water than I used to.
Once a month, I complete a Registry questionnaire. Has my quality of life improved or deteriorated? How well am I able to function? I report side effects and possible adverse reactions to the supplier as they occur and fill out their questionnaire.
I talk about CBD because I think others should know about it. People ask me whether it makes me high (it doesn’t), whether I can drive legally (depends on my ability to pass a roadside sobriety test) or visit the U.S. Over the course of the last two months, I’ve been surprised by the number of those taking CBD for a wide variety of conditions. A friend’s COPD has improved, another’s arthritic pain is less crippling. I take them for what they are — anecdotal evidence of the efficacy of CBD as an anti-inflammatory and pain reliever.
As a journalist, I have covered Canada’s transition from Killer Weed and reefer madness to legal pot, beginning with the Le Dain Commission hearings into legalization versus decriminalization. My biggest regret is that the Trudeau Liberals made legalization of recreational marijuana their priority, launching Canada into the big experiment before the medical profession is set up to measure the effects on individuals and the healthcare system. At the same time I find it beyond idiotic that Quebec doctors are still being discouraged from writing medical cannabis prescriptions and I find myself wondering what it will take to show how federal and provincial regulatory bodies are conspiring with those who manufacture, market and distribute opioids to keep patients “sweaty, fat, lazy, unmotivated — and still in pain.”
Is CBD a medical magic bullet? Which markers determine whether someone will respond well to cannabinoids and who might be genetically predisposed to psychotic or allergic reactions? Why do men and women respond differently? Without research, without scientifically conducted clinical trials, we won’t know until the U.S. jumps in — which is happening as I write this.
The Quebec Cannabis Registry is said to be planning to release details from its database this spring. In the meantime, I’ve spent the past month plowing through the contents of Therapeutic and Recreational Cannabis: In Search of Answers, an 83-page Powerpoint shown to doctors, pharmacists and nurse practitioners. It draws case histories from the Registry.
Powerpoint takeaways:
— Current knowledge of the body’s endo-cannabinoid system is fragmentary but we know it is involved in regulating the cognitive system, fertility, pregnancy, appetite, mood, pain sensations and motor learning.
The human body manufactures its own endo-cannabinoids: anandamide, which acts on the same pain receptors as THC, and 2-arachidonoylglycerol, or 2-AG, which appears to control the level of a certain fatty acid that limits body’s anandamide levels. These molecules latch onto CB1 and CB2 receptors to regulate and control a range of bodily functions. The theory is that a correct ratio of cannabis plant-derived analogs tetrahydrocannabinol and cannabidiol can help rebalance the body’s endo-cannabinoid system. But drug basics — counterindications, dosage, interactions and side effects are fragmentary.
We know there’s an individual optimal mix of THC and CBD but we don’t know much about the 140 other compounds found in cannabis strains. We’re beginning to learn about the function of terpenes — aromatic components in cannabis extracts — in modulating the effects of THC and CBD.
Research, most of it anecdotal, has determined that ratios of caryophyllene, limonene, myrcene, pinene and terpineol play a role in determining the psychological effects of different cannabis strains. The farthest the industry goes in assigning specific benefits to terpene combinations is to describe them as having an “entourage effect” — a hypothetical mechanism by which compounds in cannabis largely non-psychoactive by themselves moderate the overall psychoactive effects of the plant.
The Powerpoint’s clinical observations about CBD and THC are convincing, not only in the treatment of neuropathic pain but the generalized symptoms of pain, psychic troubles, inflammatory and auto-immune disorders and neurological complaints can be mitigated. Studies show positive results in treating of epilepsy, anorexia, fibromyalgia, inflammatory bowel and intestinal disease, chronic migraines, acute pain sensitivity, chronic fatigue syndrome, bipolar disorder, autism spectrum disorders, insomnia, anxiety, PTSD, schizophrenia and depression.
The presentation begins with a pharmaceutical history of pain relief, then shows how CBD and THC are being used to treat the same disorders with positive results. By the 63rd slide, the dissertation gets into pain-relief specifics: preliminary results from the Registry show reductions in neurological and mixed back pain, radiating lower neck pain with or without dystonia, CRPS, post-operative visceral pain (abdominal and pelvic), post-traumatic chronic headaches and migraines, jaw pain and cancer-related pain (nausea, wasting).
“We are likely going to be able to show major pharmacological benefits and savings in pain treatment,” the presentation concludes. “Most psychoactive drugs will eventually be phased out.”
This is where some of the research is concentrating — on the use of CBD to wean opioid addicts off their drugs. (This presentation was funded by Purdue Pharma and Janssen Ortho, two major opioid producers.) North America uses 80% of the world’s prescription opioids. It’s a $2.6B industry. Access to replacement treatments using methadone and suboxone is extremely limited. There is an 85% risk of relapse. Even through the genetics and neurobiology of addiction are well known, funding for research is very limited. The subject is poorly or not taught in medical schools.
Pain researchers report immediate effects when CBD is combined with opioids. Pain relief is immediate and tolerance levels are lowered. Some patients stopped taking opioids. Others stopped taking antidepressants, anti-convulsants and anti-spasmodics. “…there is evidence that CBD…can play a role not in opioid withdrawal, but with other stimulants — nicotine, cocaine, amphetamines.” Doctors currently prescribing medical cannabis agree Quebec’s pharmacies are best situated to ensure compliance and provide advice to patients about the side effects of terpene profiles.
Quebec Cannabis Registry case histories:
#3 52-year-old female with chronic back and hip pain, migraines, chronic fatigue, insomnia off work for 2+ years and walking with a cane, treated with 30 mg of CBD and 7.5 mg. THC/day. No longer uses fentenyl patches, gabapentin, naproxyn, Cymbalta, Tramacet, Elavil, clonazepam.
#4: male, 70, with progressive chronic pain since 2004, fibromyalgia, neuropathic pain in hands, chronic fatigue and insomnia, treated with CBD 30 mg/day and THC 2×23 mg/day. Has ceased taking Cymbalta, oxycodone, ketamine, Tylenol, naproxyn, OxyNeo, gabapentin, Nabilone, Elavil, Senecot/Colace.
#5: 42-year-old woman with Lynch Syndrome underwent colon, brain and breast surgeries in adolescence.Suffers from chronic head and abdominal pain. Treated with CBD and THC, she has stopped using Elavil, Constella, Effexor, dicyclomine,Prevacid, naproxyn, gabapentin, citalopram. She continues to take meds prescribed for bipolar disorder.
#6: Female, 52, with Crohn’s disease underwent total colectomy, suffers from rheumatoid arthritis, chronic abdominal pain. Medications included prednisone, Statex, Gravol, Serax, Tylenol, Pantoloc, Purinethol. Since being placed on 15 mg of CBD and 10 mg THC at bedtime, she no longer uses prescription meds.
#7: 38-year-old woman diagnosed with fibromyalgia in 2005 and spinal arthritis in 2007, was given 26.3 mg of THC at bedtime and 20 mg. of CBD twice daily. She stopped using fentanyl patch, Elavil, Cyclopenzaprine, Topamax, Dexilant, Seroquel, Lax A Day and Gabapentin. By September, she was receiving injections of Certolizumab, a biologic medication prescribed for Crohn’s and several forms of arthritis.
#8: 35-year-old mother of four suffered kidney stones and related infections. Diagnosed with psychiatric disorder, addicted to dilaudid and other prescription painkillers. Unable to tolerate methadone, she was switched to the opiod Tapenadol. She is undergoing cannabis therapy while continuing Tapenadol and the antidepressant Effexor.
#9: 32-year-old woman underwent total colectomy and ileostomy in the course of an emergency caeserian and underwent nine more surgical procedures for adhesions. Suffers from chronic abdominal pain, took to injecting prescription meds to cope. Hospitalized, she was switched from hydromorphone to metadol and is undergoing cannabis therapy to wean her from metadol. She’s off opioids dilaudid and Contin and will stop taking the tranquilizer clonazepam and Trintellix, an antidepressant.
#10: Male, 37, suffered a crushed wrist in 2015 and subsequent neuropathic pain. Unable to tolerate prescription painkillers, consumed 6-8 grammes of dried cannabis per day. Switched to 2 grammes of THC/CBD hybrid cannabis flowers and daily doses of THC and CBD oils.
#11: Female, 56, severe chronic back pain, multiple intolerances to prescription painkillers, walks with a cane with difficulty. Placed on a dosage of 1-3 grammes of a mix of CBD and THC cannabis strains, she stopped taking her daily mix — Lyrica, Kadian, Emtec, Contin, dilaudid, naproxyn, Flexeril.
#12: 60-year-old male injured his left knee in a 2005 workplace accident and was forced to stop working 10 years ago as the result of chronic neuropathic pain. Opioid dependent, he became obese. Since starting to take gelcaps of a THC/CBD oil mix at suppertime, he stopped taking Oxyneo and oxycodone and has reduced his metadol prescription by two thirds. He has since returned to work and has lost 47 pounds.
The presentation’s conclusions:
— Our lack of understanding of neuropathic pain, addiction and pain hypersensitivity has led to the misuse of opioids.
— Opioids have their place, but new restrictions must be placed on their use.
— The preliminary results of the Quebec Cannabis Registry demonstrate an efficacy inneuropathic pain, inflammatory diseases, and possibly in relieving pain hypersensitivity and the symptoms of opioid withdrawal.
— Cannabis isn’t tolerated by everyone and will not be covered until in-depth studies are published, which will take considerable time unless demonstrated savings in [drug, hospital and social costs] generate the political will to effect change.
— The Colleges [of Physicians and Surgeons] the faculties of medicine and the Order of Pharmacists should promote the teaching of these subjects to their members.
— What is considered recreational usage is often the result of self-medication for an undiagnosed condition. These individuals should be able to access the information required for healthy use of these products.
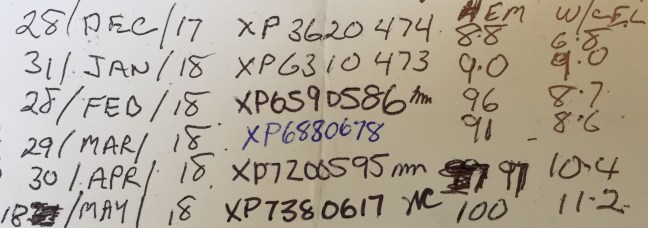
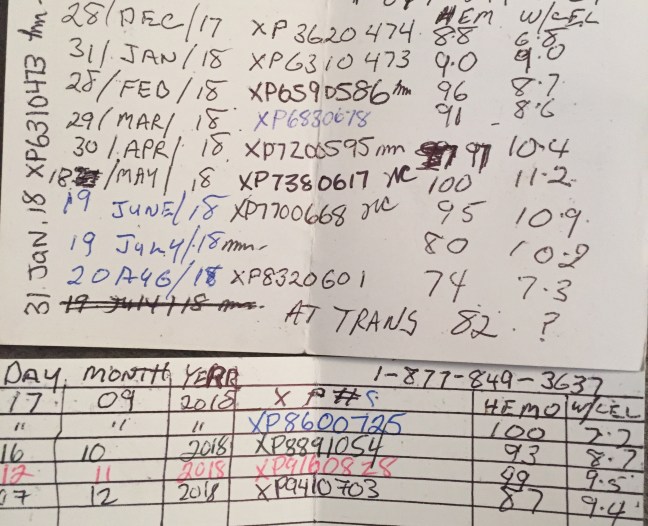
Gray keeps his monthly bloodwork results on the back of one of his hospital cards. He says it’s the only proof he needs to stop taking prescribed medications in favour of self-treatment with cannabidiol.
He’s a biker, even if his shoulder-length hair and beard are turning white and his once muscled body has wasted to lean bordering on frail. His Moto Guzzi sits in the shed, in front of the bench where he grows cannabis under LED lights. He’s smoked weed most of his life, but these “girls” as he refers to his female plants, will never be immolated. Gray says he hasn’t smoked since he began extracting cannabis oils a year ago.
Gray has MDS, myelodysplastic syndrome, a form of blood cancer. The immature blood cells his bone marrow produces don’t mature. Some patients with lower-risk forms of MDS can live five years or more. In 30 per cent of cases MDS degenerates into acute myeloid leukaemia, a form with a far shorter life expectancy.
When Gray was diagnosed with MDS, his doctor told him he had 18 months and put him on Darbepoetin to raise his hemoglobin level. For three years he received the $1,580 injections every three weeks. He was also prescribed up to eight Oxycontin tablets a day.
Three years later, Gray was barely functioning. His hemoglobin/white cell counts continued to decline. That and the Oxycontin left him wasted, so he stopped the darbepoetin and replaced the Oxy with Percocet, a combination of acetaminophen and oxycontin. Online, he’d been following the advice of Rick Smith, a Canadian cancer survivor who counsels supplanting or supplementing conventional treatments with a mix of tetrahydrocannabinol (THC) and cannabidiol (CBD) extracted from dried cannabis. Like Smith, Gray believes a THC-rich blend is more effective in killing cancer cells.
He continued to monitor his hemoglobin level and white cell count, both of which rebounded. When his cannabis extract supply ran out in October, his levels dropped so fast and far, he required two blood transfusions. Since then, he makes sure he has the raw materials to maintain a steady supply.
He’s still taking the opioid Percocet, but at lower levels than prescribed. “There are days I’ll feel like popping a perk,” he says. He believes opioids helps him function in the mornings.
He doesn’t share his self-medicating details with his doctors. “Oh, they know, but they don’t want to know.” He’s a firm believer in the conspiracy theory placing the self-regulating bodies that oversee Canadian medical professionals in bed with Big Pharma. Doctors are encouraged to continue prescribing prescription painkillers and discouraged from assisting their patients in exploring alternatives. Career-wise, it’s safer for a doctor to continue prescribing opioids despite a North American epidemic of overdose-related deaths.
A year of bloodwork has convinced Gray that a mix of CBD and THC is keeping his leukemia in check.
Long before the Oct. 17/18 legalization of recreational cannabis, the federal health establishment and its provincial agencies strove to keep the cannabis discussion focussed on regulatory issues for fear of being drawn into a larger discussion concerning the use of cannabinoids as effective, health-insurable prescription drugs.
Since 2013, any doctor in Canada is legally permitted to prescribe cannabinoids without the patient having to enrol in a clinical trial. The exception at that time was Quebec, where as of April 2014 cannabis could only be prescribed “within a research framework,” as it is not a medically recognized treatment.
To satisfy the Collège des medécins’ demand for a framework, a group of doctors and researchers announced in May 2015 the creation of the world’s first research database on the use of cannabis for medical purposes, the Quebec Cannabis Registry (www.registrecannabisquebec.com).
“We need this database to help develop and answer future questions on the medical use of cannabis, such as who uses it, for what reasons, through which methods, and at what dose.” — Dr. Mark Ware, Director of Clinical Research of the Alan Edwards Pain Management Unit at the MUHC and associate professor in Family Medicine and Anesthesia at McGill University.
The Quebec Cannabis Registry collects, compiles and store clinical data collected from patients who use medical marijuana. Participants agree to provide data for four years after recruitment. Any licensed doctor practising in the province wishing to authorize cannabis for their adult patients can thus enrol participants in the registry. The Registry’s creators set a goal of 3,000 participants over a 10-year period beginning in 2015. (It stopped taking registrants this fall after enrolling the 3,000.)
April, 2018: Quebec’s Collège des medécins cautions members against prescribing cannabinoids pending further research into efficacy, dosage and side effects. “Does one prescribe three grammes a day or five,” demands Collège secretary Yves Robert. “And five grammes of what? Cookies? Oil? Inhalation?” Doctors who prescribe cannabinoids instead of opiates had better be able to justify their choice, Robert warns.
The Collège argues that the Registry doesn’t satisfy the criteria of true scientific research and therefore can’t demonstrate that cannabinoids offer a solid alternative to opioids for chronic pain relief.
Quebec’s growing network of private cannabis clinics accuses the Collège of using veiled threats to fearmonger doctors into refusing to consider cannabis as an alternative to opioid painkillers.
Sept 20/18: Three weeks prior to the legalization of recreational cannabis, the CMQ revises its prescription protocols for medical cannabis. Quebec doctors can now prescribe cannabis outside the framework of a research project subject to the following caveats:
— A doctor must know the limits of his expertise and should not prescribe unless medically necessary.
— Based on the principle of ‘first, do no harm,’ the doctor must also ensure that a prescription’s therapeutic benefits must outweigh undesirable potential effects and risks such as dependency.
— Cannabis must not be the first treatment choice. Before considering it for treatment of a medical condition, the doctor must ensure that the patient’s response to other treatments is inconclusive. The doctor must make note of treatments tried and deemed ineffective by the patient.
— The doctor must become aware of policies regarding the use of cannabis for medical purposes as listed on the Health Canada website. The prescription of cannabis isn’t appropriate for anyone under the age of 25, anyone presenting a risk or history of dependancy, those with a family history of psychosis, anyone with cardiovascular or respiratory disease, women breastfeeding, expecting or hoping to be. The doctor must also weigh the risk to ex-smokers of prescribing inhaled cannabis.
— Upon prescribing, the doctor must carry out a full medical evaluation, in person, and must note the patient’s free and informed consent in his file. He must inform the patient of possible effects and complications on the patient’s health (depression, psychosis, mental illnesses, lung disease, connitive decline, memory loss, reduction in professional or scholastic performance). — The patient must be aware of his responsibilities in following this treatment, specifically while driving and preventing the drug’s use by minors.
— The patient must schedule visits to the doctor as needed to ensure adequate followup of his medical condition. A first followup visit should take place within three months of the initial prescription depending on the clinical conditions and until the stabilization of the patient.
The patient must not sell or traffic in prescribed drugs.
— The doctor must cease prescribing cannabis in the event of a complication or if the patient doesn’t fulfill his obligations.
— Treatment must begin with the lowest possible dose and increases must be managed with care.
— In all cases, treatment must be signalled to the the treating physician as well as to other doctors following the patient with the patient’s consent.
— The doctor must note in the patient’s file the indication for which the cannabis is prescribed.
— The doctor must keep a register of patients for whom he has prescribed cannabis so as to permit control and adequate followup of his clientele and rapid access to files.
The CMQ protocol also addresses potential conflicts of interest:
The authorization or prescription for the use of medical cannabis or supplementary fees cannot be billed by the physician. The doctor cannot derive profit from prescribing medical cannabis and cannot directly sell or provide it to the patient.
— The prescribing physician must allow the patient the freedom to choose a supplier.
— The physician must safeguard his professional independence at all times and avoid any situation in which he would be in a conflict of interests. To this end, if the physician has financial interests in an enterprise engaged in the production of cannabis, must so inform the patient as well as the milieu where he practices.
Pain specialists expressed disgust at the CMQ’s latest edicts, arguing that opioids, with their known risks of addiction and abuse, are the real problem. Research has shown phytocannabinoids THC and CBD can work in harmony with the body’s own endocannabinoids to mitigate pain. “The pharmeconomy would save millions, maybe billions, in drug and treatment costs with cannabinoids,” a Quebec GP told me.
October 2018: The Quebec Automobile Insurance Board refuses to reimburse the cost of cannabinoids prescribed as a cost-effective pain treatment alternative to opioids such as dilaudid, fentanyl and methadone. Only medications bearing a DIN and listed in the Régime général d’assurance médicaments (RGAM) are reimbursable. (CNESST, Quebec’s workplace health and safety agency, will consider reimbursing the cost of prescribed cannabinoids.)
Of the provinces, Quebec maintains the hardest stance on cannabis. The current government proposes to raise the legal consumption age to 21 regardless of the federal legal age, 18. Quebec is the only province to ban unlicenced cannabis production (not even the federally sanctioned four plants), yet outlets of the SCDQ, the provincially managed cannabis marketing structure, are closed half the week for lack of product. Who benefits from that?
Gold-rush hucksterism
This past April, I attended a cannabis industry conference in Montreal and blogged about it (https://thousandlashes.ca/2018/04/16/cannabis-update-risk-vs-potential/). Major producers Canopy Growth, Aurora and Hypothecary were there, along with Health Canada and a jam of lawyers and lobbyists — regulatory and governance specialists, branding and trademark lawyers, M&A suits. I met venture capitalists and insurance actuaries, producers and foodies.
Researchers provided a reality check to the gold-rush huckerism. A mid-morning panel on the scientific and medical implications of legalization featured McGill’s Dr. Mark Ware, the Université de Sherbrooke’s Dr. Serge Marchand and New Brunswick Health Research Foundation head Dr. Bruno Battistini. They foresaw serious public health issues resulting from Canada’s legalization of the recreational use of cannabis, at that point still six months away. Their biggest concern —the 20 per cent of recreational pot users at risk of mental illness. THC, the psychoactive component of cannabis, latches onto receptors in the brain that trigger certain pleasure reflexes. This 20% is at risk of developing psychotic reactions, especially among adolescents and young adults.
The panel stressed the need for extensive research into phyto-cannabinoids, the collective label given to 142 molecules found in various cannabis strains. The two best-known cannabinoids are delta-9-tetrahydrocannabidiol, or THC, and cannabidiol, or CBD. THC is responsible for many of the pharmacological effects of cannabis, including the psychoactive effect — the high. CBD doesn’t have any of the intoxicating, euphoric effects of THC.
The researchers described CBD’s potential as a medical ‘magic bullet.” Cannabidiol is being used to treat a growing list of conditions — Crohn’s and other inflammatory bowel diseases, PTSD and other psychological disorders, fibromyalgia, rheumatoid arthritis, epilepsy, MS, Parkinson’s, Alzheimer and dementia, austism spectrum disorders, acne — and opioid addiction. But without clinical trials and scientific methodology, the medical cannabis industry can’t advance past the anecdotal stage and opiates will remain North America’s default prescription painkillers despite their toxicity and potential for abuse.
Ware, who has since gone on to become chief medical officer for Canopy Growth, is a West Island family doctor who co-founded the Canadian Consortium for the Investigation of Cannabinoids (CCIC) while serving as director of clinical research at the MUHC’s Alan Edwards Pain Management Unit. He described how difficult it was to convince doctors to enrol their patients in cannabinoid clinical trials because of resistance from the profession’s governing bodies. (To get around Quebec’s Collège des médecins and its convoluted protocol for the prescribing of cannabinoids, Ware and a group of pain specialists in May 2015 launched the Quebec Cannabis Registry (www.registrecannabisquebec.com), the world’s first research database on the use of cannabis for medical purposes. In late 2018, registration was closed at 3,000 patients.)
Drs. Ware, Marchand and Battistini concluded on a down note: In legalizing recreational weed, Canada has opened the door to cannabis’s medical applications. However, they warned, it was a matter of time before the U.S. removed CBD from the DEA’s list of Schedule 1 drugs (no currently accepted medical use, high potential for abuse). Once that happens, Canada would lose its advantage.
As they predicted, the U.S. Drug Enforcement Administration five months later moved CBD from Schedule 1 to Schedule 5, allowing the prescribing and sale of CBD-derived formulations with levels of THC below 0.1%. In December, the Hemp Farming Act of 2018 was signed into law, making CBD a legal agricultural product. Estimates peg the U.S. CBD market at $23B annually within 10 years.
Equally sudden has been the opioid backlash directed at producers and distributors. In the U.S. the attorneys-general of 41 states have served five major opioid producers and three distributors with subpoenas seeking information about how these companies marketed, sold and distributed prescription opioids. Civil class-action lawsuits alleging the industry misrepresented the effectiveness and addictive nature of opioid painkillers are being filed across America.
In Canada, the opioid backlash so far has been limited to B.C., which in August announced it would file a class-action lawsuit against dozens of players in the opioid industry. The province’s attorney-general alleges 20 years of misinformation and deception about the effectiveness and risks of addiction and asked other provinces to join B.C.’s action. Although a number of provinces with their own skyrocketing opioid-overdose death rates said they would review B.C.’s action with an eye to joining it, none have stepped forward.
Why the silence? None of the professionals I spoke with wished to be quoted, but they generally agreed the problem lies with Canada’s medical insurance structure. Public and private insurers buy in bulk from the distributors, who motivate doctors and pharmacists to prescribe.
Are opioids effective, non-addictive painkillers when used as prescribed? Here’s what one Quebec pain and addiction specialist told me: “I came to realize that my patients taking opioids for pain relief were fat, lazy, sweaty, non-functional — and still in pain.” The condition is called opioid-induced hyperalgesia, characterized by a paradoxical response whereby a patient receiving opioids for the treatment of pain could actually become more sensitive to certain painful stimuli.
Urinalysis and close questioning led to his discovery that some of his pain patients were trading their prescribed drugs for more powerful alternatives. Others were selling all or part of their prescription for cash. His doctor-patient relationship prevented him from turning them over to the police. The response from the Quebec Collège des médecins? Stop prescribing.